

Kerala, often heralded for its efficient healthcare system and robust basic facilities, stands as a beacon of health infrastructure within India. Yet, despite its healthcare prowess, an unsettling truth prevails: migrant workers often encounter insurmountable barriers when attempting to access essential healthcare services. While Article 19 of the Indian Constitution endows citizens with the freedom to move and work across the nation, a deeper inquiry reveals that realising this fundamental right necessitates a proactive and multi-faceted engagement from local self-governments.
The heart of the matter is in the fact that the health system, despite its merits, is often non-accessible to migrant laborers. The dynamics of migrant labour reveal the dichotomy between constitutional rights and the real-world challenges encountered by those striving to secure a livelihood. The vision of India as a nation where citizens can freely traverse its territories to pursue employment opportunities is indeed noble, but its realisation demands a more comprehensive approach.
An avenue for addressing the intricacies of this issue lies in the role of local self-governments. While the Constitution provides the framework, it is the local governance bodies that must proactively engage in social interventions. These interventions are paramount to establish just policies and institutional frameworks that align with the spirit of Article 19. An intricate balance between mobility and accessibility must be struck, recognising that the aspiration for economic betterment should not come at the cost of basic human rights, including healthcare.
READ I Soaring outward remittances may help India expand its financial footprint
Public health access for migrant workers
Delving into the core challenges faced by migrant workers reveals a landscape riddled with obstacles. For those engaged in interstate labor, the irony emerges – the very government health facilities that could provide solace often remain inaccessible due to operational hours mirroring their work hours. This intricate overlap renders taking a day off for health-related visits a dilemma. Even a willing sacrifice of a day’s wage cannot always compensate for the repercussions faced in terms of livelihood and sustenance.
The lack of awareness about local health facilities compounds the issue. In places like Perumbavoor in Kerala’s Ernakulam district, where migrant workers are prevalent, a disheartening reality unfolds. The existence of undocumented doctors who cater to the healthcare needs of these migrants speaks volumes about the gap in accessibility to established healthcare institutions. This further propels the demand for an integrated approach where local governments play a proactive role in bridging these gaps and providing a safety net for the labor force.
The predicament of plantation workers, often neglected in discussions on labor, demands attention. Their plight is exacerbated by the absence of government health facilities in proximity. The underprivileged state of these workers underscores the need for their employers to take on the role of healthcare providers, a role they may be ill-equipped to fulfill. This dependence on employers for healthcare further emphasises the need for systemic solutions that move beyond ad-hoc arrangements and establish a framework for equitable access to healthcare.
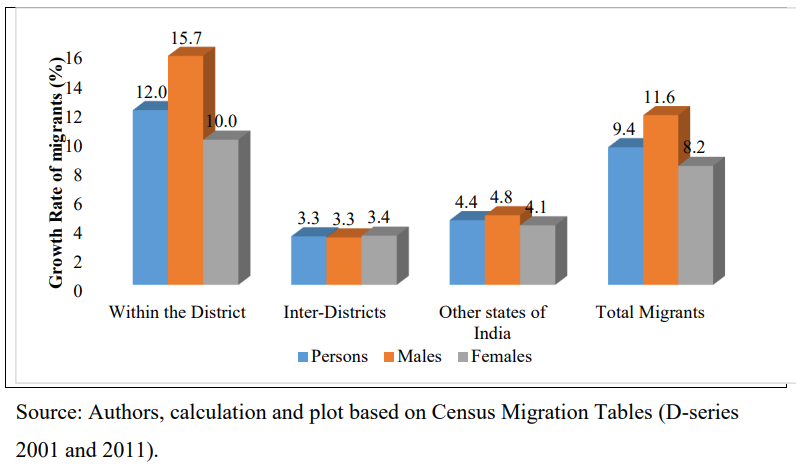
Annual growth pattern of migration into Kerala
Language emerges as a significant yet overlooked barrier. Effective communication between healthcare providers and non-Hindi-speaking or even Hindi-speaking workers becomes a challenge. The convergence of rushed medical facilities and linguistic barriers impedes accurate diagnosis and limits the potential for effective healthcare delivery. In essence, the quest for equitable healthcare demands not only physical accessibility but also communication that transcends linguistic confines.
Another alarming issue arises from the act of self-treatment among migrant workers. Despite receiving prescriptions, the practice of bypassing recommended medical tests in favor of pharmacy-bought medications exacerbates health risks. This phenomenon not only challenges the health of migrant workers but also underscores a broader need for health literacy and awareness campaigns targeting this vulnerable demographic.
The overarching narrative reveals that even in emergencies, migrant workers are not immune to neglect. Instances abound where these workers are denied immediate care due to a lack of bystanders or an inability to pay medical bills upfront. The transient nature of their work, compounded by language barriers, often leads to inconsistent adherence to treatment. The challenges faced by migrant workers in treating diseases come to the forefront, revealing a complex web of factors that hinder continuity in medication and care.
Migrant women more vulnerable
The challenges magnify significantly for migrant women, who find themselves embroiled in an array of obstacles. Often working in informal sectors, these women confront unsafe work conditions, inadequate nutrition, and insidious discrimination. The link between working conditions and maternal health becomes strikingly apparent. Unhealthy work conditions, including prolonged standing and bending, expose pregnant women to elevated health risks. The lack of nutritious food and inadequate care during pregnancy further compounds these challenges, potentially leading to adverse maternal and child health outcomes.
Moreover, the vulnerability of migrant women extends beyond just physical health risks. As per a 2013 report by UNESCO and UNICEF, migrant women often grapple with poor maternal and child health outcomes, accompanied by an increased susceptibility to sexual abuse, exploitation, and violent incidents. These dire challenges stem from the disadvantaged socioeconomic circumstances that permeate both the individual and household tiers of migrant women’s lives.
In a broader context, studies indicate that migrant workers are also at risk of diseases like HIV/AIDS due to a lack of awareness about disease transmission and safe sexual practices. Mental and physical health issues emerge as significant consequences of the departure from native social setups, compounded by the realities of their new work environment. Factors such as dietary changes and shifts in physical activity patterns contribute to the vulnerability of migrant workers to these health risks.
However, amid these multifaceted challenges, a glimmer of hope arises in the form of the “Kerala Public Health Bill-2021.” This legislative initiative, introduced in the state’s legislative assembly, proposes the establishment of a three-tier public health governance system. Designed to replace the Thiruvithamkur-Kochi public health act (1955) and the Madras public health act (1939), this bill charts a course towards a comprehensive transformation of the state’s public health landscape.
The proposed bill not only underscores the containment of transmittable and non-transmittable diseases but also prioritises adequate water supply and proper waste management – critical components in ensuring a healthy populace. The focus on providing sanitised living conditions and safe workspaces carries special relevance for migrant workers, who often inhabit poorly sanitised dwellings. Moreover, the bill’s emphasis on a decentralised three-tier panchayat system holds promise in addressing the unique needs of migrants, Adivasis, and marginalised populations. By incorporating these considerations into policymaking and program implementation, the bill strives to foster a more inclusive and equitable public health environment.
Kerala’s lauded healthcare system stands as a testament to the possibilities of a robust health infrastructure. Yet, the challenges faced by migrant workers in accessing healthcare expose a rift between constitutional rights and on-ground realities. The complex interplay of language barriers, inconsistent adherence to treatment, and the vulnerabilities faced by migrant women underscores the pressing need for comprehensive solutions.
The Kerala Public Health Bill 2021 emerges as a beacon of hope, presenting an opportunity to reshape the state’s health governance and prioritise the welfare of migrant workers, Adivasis, and marginalised populations. Through proactive local governance and inclusive policy frameworks, Kerala has the chance to pave the way for equitable healthcare access and uphold the promise of Article 19 for all citizens, irrespective of their mobility.
(Navas M Khadar is Project Associate, GOI-SERB Project on Interstate Migrant Workers, School of International Relations and Politics, Mahatma Gandhi University, Kottayam. Jose Deepak TT is a Scholar at Indian School of Public Policy, New Delhi.)