

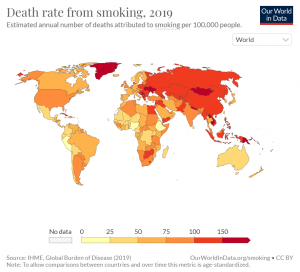
India’s tobacco regulation suffers in the absence of holistic solutions based on scientific evidence. In India, more than 1.5 million people die every year due to tobacco consumption. Tobacco is the single most important cause of premature mortality and harm reduction is gaining currency across the world as a strategy to reduce the levels of mortality. The underlying philosophy of harm reduction is pretty simple — as it is difficult to wean smokers away from tobacco, provide them with less harmful products containing nicotine.
India banned all harm reduction products in 2019 under the Prohibition of Electronic Cigarettes (Production, Manufacture, Import, Export, Transport, Sale, Distribution, Storage, and Advertisement) Act. Three years into the ban, the market is flooded with all kinds of illegal products. There is growing concern about their use among young children. As these products are available across the country despite the ban, there is a need for scientific assessment of their health impact.
The ban on harm reduction was made on the recommendations of a study conducted by the Indian Council of Medical Research in 2019. The ICMR study was comprehensive, but it could not have covered data after 2017. This means there is a need for studies that cover data from the last five years.
READ I ‘Harm reduction is the future of tobacco regulation’
Tobacco harm reduction a divisive topic
The discussion on harm reduction must take a dispassionate view without taking sides. The biggest problem with the ongoing debate is that policymakers, non-profits, and self-help groups are sharply divided on the subject. No one seems to be interested in listening to others or look at the emerging evidence on the subject.
Smoking appears to be more harmful than vaping and other harm reduction methods, but this does not mean that these methods are totally safe. But isn’t that the case with most of the medicines that we take regularly? Oncologists will admit that chemotherapy has major side-effects, but they use it whenever required. Psychiatrists will vouch that tobacco addiction is a chronic medical condition. It is a pandemic that kills millions and causes sufferings for millions of others.
Now, let’s take a look at the data from across the globe. Around 70% of the smokers are interested in quitting and around 50-60% actually try to quit. Unfortunately, only about 7.4% of them manage to quit the habit. There is a less than 10% success rate. So, it makes sense to look at tobacco harm reduction as a public health opportunity.
Harm reduction can be one of the pillars of cessation assistance. Many in the medical profession have not had a look into the aspect of harm reduction. Harm reduction is controversial and so they look at the concept with scepticism. The purpose of harm reduction is well-known and one could discuss it when there is time. The environment is conducive now as the tobacco industry is publicly acknowledging the dangers of smoking.
It could be that the tobacco industry is accepting that their products cause harm because they are forced to. They now accept that smoking kills their consumers and that they probably have to move away from these products. There are novel products which address concerns. Here, public health concerns merge with the business interests of the industry. The quit-or-die situation necessitates policy action.
The worst thing that could happen to harm reduction is the use of modified tobacco like light cigarettes. This was the biggest disaster for tobacco harm reduction. The industry used this as a sort of cover to sell more cigarettes. By the time everybody realised that people were hooked, there had already been deaths. This led to a general distrust in anything that is called safe.
Do we have products that can lead to lesser harm? The biggest category here is e-cigarettes. England regards it as one of the techniques of cessation for people who cannot quit despite many efforts. There will also be someone who will say that it is their right to smoke and that they do not want to quit. Is there something to offer such people? Or do we say simply ban tobacco products? Such a person could continue smoking and die. We cannot reduce the harm done to their health. This is the situation we need to understand. A lot of data has been published by big journals in the last two years in support of tobacco harm reduction.
There is a huge amount of data that supports substitution of cigarettes with less harmful products, but there is no concluding evidence that harm reduction products are totally harm free. So, one cannot recommend them for everyone. But if a patient is unable to quit and it is clear that smoking will definitely harm, these products should be allowed under the doctor’s watch.
Different studies show that the impact of e-cigarettes on the heart and circulation is less than that of conventional cigarettes. This is a whole spectrum of harm reduction — combustible tobacco products are the most dangerous, followed by chewing tobacco products. The least dangerous products are NRT because they are like substituting nicotine. Harm reduction products are somewhere in between.
The problem here is acceptance. NRT is available in all our programs and available over the counter. What are the sales? There are hardly any companies who want to come out and they don’t promote it to doctors. There is a company which makes lozenges but when it came to prescribing it for patients, the product was just not available. It is probably given out only to cessation clinics. What will other smokers do?
Finally, the biggest chunk of the ICMR study was devoted to the subject of e-cigarettes becoming a gateway to smoking for the youth. The latest data from across the world do not uphold these findings.
There is little change in the prevalence of smoking among the age group of 16-19. If e-cigarettes act as a gateway, the number of new smokers should have increased. It is probable that the smokers were quitting and using vapes. The number has remained the same. The same studies show that the prevalence of vaping is around 7.7%, the same as 7-8 years ago. So, the argument that vaping is a gateway to smoking does not hold water.
A multidisciplinary approach is needed on harm reduction as it is not possible for a doctor with one specialisation to make a call. But a discussion with people not willing to find a common ground will not yield results. Medical professionals are taught to read and change their beliefs. They have done so in the case of many diseases over the years. Doctors need to find a middle ground, if they want evidence-based policymaking.
Prevention of initiation is the best strategy towards successful tobacco regulation. However, governments across the world have failed in prevention which requires a complete ban on tobacco products. The governments have their own compulsions as tobacco is a huge source of revenue to them. As one cannot expect a complete tobacco ban, assistance with cessation is the next best option. This is why the government must approach the subject with an open mind.