

Ebola outbreak tests global health diplomacy: The Democratic Republic of the Congo’s situation report for 8 July recorded 1,792 confirmed cases of Ebola disease caused by the Bundibugyo virus and 625 deaths. Uganda’s tally stood at 20 confirmed cases and two deaths on 10 July. France has reported one infection in a doctor who returned from the DRC.
The current outbreak is the largest recorded caused by the Bundibugyo virus. The World Health Organisation has declared it a public health emergency of International Concern on May 17. It did not classify the outbreak as a pandemic emergency, and continues to assess the global risk as low. There is no approved vaccine or specific treatment for this virus. WHO emergency-listed the first molecular diagnostic test for the virus on 2 July.
READ I US withdrawal from WHO is a strategic health failure
Bundibugyo Ebola outbreak meets eastern Congo’s wars
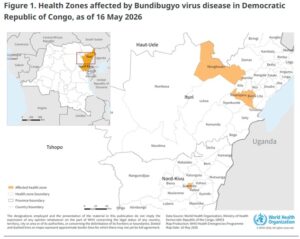
The epidemic has erupted in the Ituri province, which witnessed 1,631 of the DRC’s confirmed cases and 535 deaths on July 8. North Kivu had reported 158 cases and 89 deaths. Three cases had been confirmed in South Kivu. Thirty-seven health zones were affected.
Ituri borders Uganda and South Sudan. Its mining settlements draw mobile workers, while conflict has displaced more than a million residents within the province. The affected areas also contain trade routes, refugee communities and settlements with poor access to water and medical care. These are ready-made gaps in surveillance.
Eastern Congo’s violence cannot be reduced to a single rebellion. AFC/M23 controls territory in parts of North and South Kivu. Ituri has suffered attacks by other armed groups and communal militias. The conflicts restrict travel, close health facilities and make it harder for medical teams to reach villages. UN agencies have documented persistent armed-group violence in Ituri and North Kivu, along with attacks on civilians and obstruction of humanitarian access.
The effect can be measured. Congolese teams were following 11,927 contacts on 8 July, but had reached 9,376, or 78.6 per cent. In Ituri, the follow-up rate was lower at 76.1 per cent. Every missed contact leaves a possible transmission chain outside the response system. WHO has also reported security incidents affecting health facilities and disrupting surveillance and treatment.
Uganda presents a different picture. Fifteen of its 20 confirmed infections were imported from the DRC and five arose among contacts or health workers. WHO had found no community transmission in Uganda, while its health ministry reported no active contacts under follow-up on 10 July. Uganda faces cross-border exposure, but not an epidemic on the DRC’s scale.
READ I Hantavirus outbreak calls for stronger zoonotic preparedness
Ebola security measures need public consent
A PHEIC allows WHO to coordinate an international response under the International Health Regulations. It is not a licence for general border closures or indefinite restrictions. WHO’s temporary recommendations require governments to respect dignity, human rights and fundamental freedoms. It has advised against general restrictions on travel or trade with the DRC and Uganda.
The West African epidemic of 2014 showed how coercion can damage outbreak control. Liberia’s government sealed the West Point neighbourhood of Monrovia. Clashes between residents and security forces left a child dead and several people injured. Mistrust in parts of Guinea also led residents to resist health teams and disinfection drives.

The lesson is narrower than a rejection of quarantine. Isolation and movement restrictions may be necessary when exposure is established. But they require a legal basis, medical supervision, food and income support, time limits and a means of review. A family that expects punishment or abandonment has an incentive to conceal illness.
Patients’ rights also have an epidemiological purpose. Access to treatment, confidentiality and protection against discrimination encourage early reporting. Community leaders can help health teams identify contacts, organise safe burials and correct rumours. Soldiers may protect treatment centres and supply routes. They cannot substitute for doctors, local health workers and trusted public communication.
READ I HMPV outbreak: A wake-up call for India’s public health services
What BRICS can do in the Ebola outbreak
BRICS now has 11 members, while Uganda is one of its partner countries. Yet BRICS has no permanent secretariat, constitutive treaty or common budget. It cannot command an emergency operation or replace the DRC and Ugandan health ministries, Africa CDC or WHO.
It does have institutions that could be used. The BRICS Vaccine Research and Development Centre is operational, and the grouping has established a network of public health institutes. Members have laboratory capacity, vaccine platforms, pharmaceutical production and experienced medical teams.
A BRICS programme should assign specific work. Member laboratories could support diagnostic validation and external quality assurance. Public health institutes could provide field epidemiologists and infection-control specialists. Research centres could agree on candidate vaccine and therapeutic protocols so that trials can begin when products are ready. Governments could finance protective equipment, treatment centres and cross-border surveillance through their national aid agencies.
The bloc should make no promise of an immediate vaccine. Candidate development and trials will take time. Laboratory testing, supportive care, contact tracing and safe treatment facilities remain the available tools. WHO’s emergency listing of the first Bundibugyo molecular test has eased one constraint, but access and laboratory capacity remain uneven.
China has sent medical personnel and emergency assistance to the DRC and the African Union. It has described this support under China-Africa cooperation rather than as a BRICS operation. Calling bilateral assistance a bloc initiative would overstate what BRICS has done.
BRICS health ministers supported WHO-led action during the 2014 Ebola epidemic. The present outbreak requires more than another declaration. A useful decision would name the participating laboratories, personnel, supplies, funding and deployment dates.
Kerala’s Ebola test offers a narrow lesson
India has a relevant example. During a recent Ebola scare, the Rajiv Gandhi Centre for Biotechnology in Thiruvananthapuram tested a sample sent from Kozhikode within 12 hours. It produced a preliminary negative result in four hours, before final confirmation arrived from Pune.
The test did not “prevent an outbreak”, as some accounts claimed. It shortened the period in which Kerala’s health authorities were operating without a diagnosis. That allowed them to take decisions without waiting for a distant reference laboratory.
RGCB has a Biosafety Level 3 facility equipped for research and diagnostic development involving serious pathogens. Such regional capacity is useful when laboratories follow national standards, use quality-assured assays and report results into the official surveillance system.
This is where India can make a practical BRICS contribution. It can offer laboratory expertise, training and support for diagnostic networks while working through WHO, Africa CDC and the affected governments. The response does not need a new command structure. It needs existing institutions to deliver faster.
The DRC’s figures show where the failures lie: cases are still being found late, contacts are being missed and conflict is obstructing health teams. BRICS will be useful only when it attaches named institutions and deadlines to its offers of help. Otherwise, the outbreak will remain the responsibility of agencies already working with too little time and access.
READ I Palliative care gap is a public health failure

Dr Joe Thomas is Global Public Health Chair at Sustainable Policy Solutions Foundation, a policy think tank based in New Delhi. He is also Professor of Public Health at Institute of Health and Management, Victoria, Australia. Dr Thomas was the founding Secretary General of the Global Commission on Ageing in developing countries. He is an author of reports from seven PPD member countries documenting the ageing situation, health and well-being, and policies to enable and support environments.