

Palliative care reduces pain, distress and family burden across the course of serious illness. In India, it is still too often pushed to the last days of life. That delay leaves patients with hospital procedures after curative treatment has stopped helping, while families absorb bills, care work and avoidable suffering.
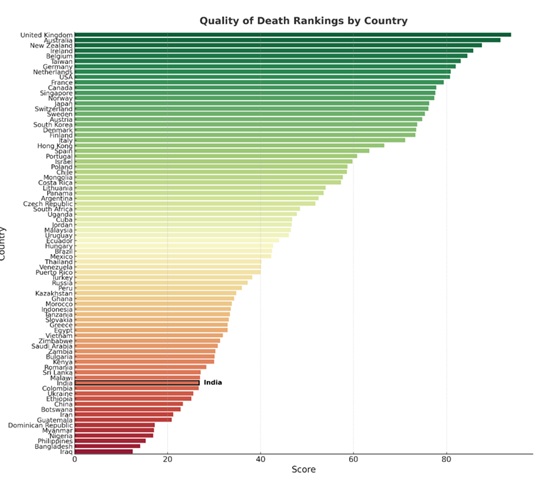
India’s international standing is poor. The Economist Intelligence Unit’s 2015 Quality of Death Index placed India 67th out of 80 countries, with a score of 26.8 out of 100. A later Quality of Death and Dying study by Eric Finkelstein and colleagues put India 59th among 81 countries, but the two rankings used different methods and cannot be read as evidence of improvement. They point in the same direction: palliative care remains outside routine care for most Indians.
Universal health coverage means less if severe pain, home care and family support reach only those who can find a charity, a rare public programme or a trained doctor.
READ I Medical titles debate raises public health concerns
Quality of Death Index and palliative care gap
The Quality of Death Index 2015 assessed countries on palliative and healthcare environment, human resources, affordability, quality of care and community engagement. The UK led the rankings with 93.9, followed by Australia at 91.6 and New Zealand at 87.6. India fared poorly, and was placed between Malawi and Colombia in the bottom half of the list.
Income explains part of the ranking, but not all of it. Mongolia, Uganda, Cuba and Costa Rica did better than income alone would predict. India’s poor score reflects more prosaic failures: too few trained professionals, weak public integration, poor morphine access and a thin community-care base.
Morphine remains the simplest test. The World Health Organisation lists morphine as an essential medicine and describes it as a basic requirement for palliative care. Yet India’s palliative care centres do not reliably provide it. A pain-relief system that cannot deliver morphine to patients with terminal illness has failed at the first step.
READ I Fertility decline: India is ageing before prosperity
Kerala palliative care model
Kerala is the exception. Its palliative care did not begin as a hospital product. It grew from community organisations, local volunteers and the Neighbourhood Network in Palliative Care, with institutions such as the Institute of Palliative Medicine in Kozhikode giving the movement clinical depth.
Kerala’s state policy later absorbed this civic base rather than replacing it. The Kerala State Palliative Care Policy 2019 focused on local governments, community organisations and home-based care. It also proposed ward-level neighbourhood networks, better access to medicines, training, accreditation and a palliative care grid.
The newer Universal Palliative Care Programme keeps the same grammar: trained volunteers in neighbourhoods, ASHA-led ward teams, home-care teams in panchayats and municipalities, secondary units in public systems and registration of NGOs and volunteers. This is administrative work, not sentiment.
READ I India’s ageing population demands a universal pension plan
Palliative care in India is uneven
A directory-based analysis of Pallium India listings counted 911 palliative care institutions across India. Nearly one-fifth offered no recorded facility across outpatient care, inpatient care, home care or morphine access. Only 20.6% offered all four. Morphine was available in 48.8%.

Kerala accounted for 244 of the 488 institutions with home care, more than half the national total. In outpatient care, Kerala had 189 facilities against Maharashtra’s 39. In inpatient care, Kerala had 106 against Tamil Nadu’s 33.
Large parts of India have no organised palliative care infrastructure. The difference between Kerala and the rest is not a matter of marginal improvement. It is the difference between a service system and scattered provision.
Kerala’s palliative care gaps
Kerala’s lead should not be mistaken for completion. District-level data show uneven coverage. Ernakulam and Kozhikode are better served; Kasaragod, Thrissur and parts of central Kerala lag. Statewide, 29.9% of Kerala’s listed institutions offered no recorded facility across the four indicators, higher than the national share in this dataset.
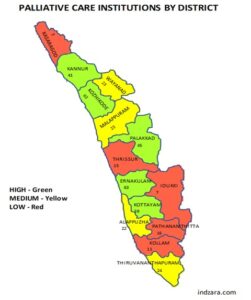
That paradox is useful. Kerala is India’s best model, but it still has service gaps, weak districts and uneven institutional capability. Its example should be studied without turning it into a slogan.
Aggressive end-of-life care raises costs
Palliative care is not an argument against treatment. It is an argument against futile treatment when suffering, dignity and family burden are ignored. Evidence from palliative care research, including the Lancet Commission on the Value of Death, shows that better palliative care can improve outcomes for patients and carers, often at lower cost. Studies on early palliative care also link it to lower health-system costs near death, largely through fewer avoidable hospitalisations.
India’s default is often the worst of both worlds. Curative care continues when it no longer cures. Supportive care arrives late, if at all. Families pay for procedures, travel, medicines and lost work while the patient’s pain is poorly managed.
India’s palliative care policy choices
India did not start from a blank page. The country launched its National Programme for Palliative Care in 2012. Operational guidelines for Health and Wellness Centres link palliative care to universal health coverage. The National Health Policy 2017 also recognised palliative and rehabilitative care. The problem is that these have not become a funded, measurable service guarantee across district hospitals, primary health centres, Health and Wellness Centres and home-care networks.
The first task is to put palliative care inside the public health system. ASHAs, community health officers, primary health centres and district hospitals should identify patients early, refer them properly and support home care. This cannot remain dependent on a few NGOs and motivated doctors.
The second is morphine access. Parliament amended the NDPS Act in 2014, and the National Programme for Palliative Care already exists. Even so, licensing, storage rules, paperwork and fear among hospitals continue to restrict use. Reform has to reach the pharmacy counter and the bedside.
The third is training. Palliative care belongs in undergraduate medical and nursing education, not only in specialist courses. Oncology, cardiology, neurology, geriatrics and respiratory medicine should refer patients before crisis admissions begin.
The fourth is community capacity. Kerala shows that volunteers are not an accessory to palliative care. They are part of the infrastructure. Replication elsewhere will need local governments, ward-level mapping, public health staff, accredited NGOs and money. Civil society cannot carry a national obligation alone.
Cancer, cardiovascular disease, chronic respiratory illness, dementia and kidney failure will increase demand for palliative care. WHO identifies cardiovascular disease, cancer and chronic respiratory disease among the major conditions driving adult palliative care need. India’s ageing population will add to that load.
Kerala should fix its district gaps before claiming universality. The rest of India has less excuse. It has the National Programme for Palliative Care, Health and Wellness Centre guidelines, the NDPS amendment and Kerala’s example. Patients still lack a service they can find, afford and trust.
Dr Hari Kurup KK is Director, Institute of Surveys and Studies, Thiruvananthapuram.