


In 1954, a British doctor warned that humanity might soon “run clean out of effective ammunition” against bacterial infections. That grim prophecy has come true. More than 70 years later, the United Nations calls antibiotic resistance “one of the most urgent global health threats”. It already claims over a million lives each year—more than malaria or HIV/AIDS—and the toll could climb exponentially unless decisive action is taken.
Unlike other medicines, antibiotics do not just affect the patient who consumes them. Every use shapes the microbial environment, raising the likelihood that another person’s infection may no longer respond to treatment. The thesis is inescapable: antibiotic resistance is not a marginal challenge for hospitals or laboratories; it is the greatest threat to human health, one that could dismantle the very foundations of modern medicine.
READ I Ukraine peace hinges on Europe scaling back militarisation
Why antibiotic resistance
Paracetamol relieves pain by altering chemical signals in the body; insulin regulates blood sugar; statins lower cholesterol. These medicines act on human biology. Antibiotics, by contrast, act on bacteria. But bacteria multiply and spread, exchanging genetic material with remarkable speed. That means misuse or overuse of antibiotics by one individual can make infections untreatable for another.

The analogy with fossil fuels is striking. Both are natural resources, discovered rather than invented. Both created an illusion of endless abundance. Just as coal and oil powered industrial revolutions, antibiotics powered the medical revolution—making safe surgeries, organ transplants, cancer chemotherapy, and intensive care possible. Both, however, have been dangerously overused, generating pollution in the case of fossil fuels and resistance in the case of antibiotics. In Hyderabad, wastewater from factories producing antibiotics contains concentrations a million times higher than natural background levels.
The superbug menace
The threat is no longer theoretical. Resistant bacteria have breached frontline hospitals across the world. Methicillin-resistant Staphylococcus aureus (MRSA), multidrug-resistant tuberculosis (MDR-TB), and penicillin-resistant Enterococcus are among the best-known. MDR-TB alone is a public health nightmare: it requires toxic, prolonged, and expensive treatment, and often gives rise to extensively drug-resistant TB that borders on untreatable.
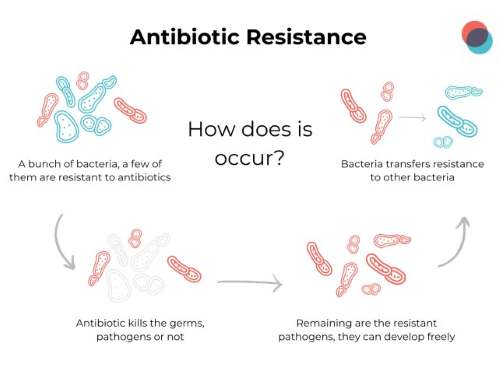

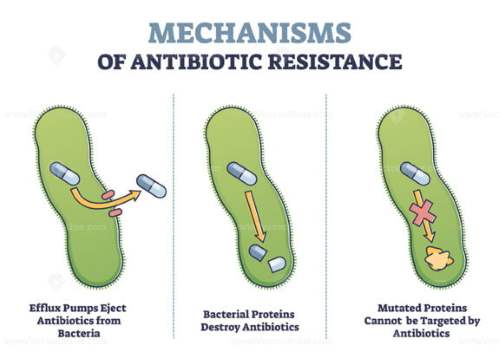
The biology of resistance explains the scale of the challenge. Bacteria evolve rapidly through mutation and genetic exchange. They share resistance genes via plasmids, transposons, and bacteriophages. Once a resistance trait appears, it spreads like wildfire across species. Antibiotics do not create resistant strains; they merely apply the selective pressure that allows them to dominate. This explains why resistance has been reported for nearly every antibiotic within a few years of its introduction.
Market failure and policy paralysis
Despite the crisis, pharmaceutical innovation in antibiotics has nearly collapsed. Most antibiotics used today were discovered more than 60 years ago. The economics are brutal: antibiotics are taken for short courses, unlike drugs for chronic diseases. Worse, every use of a new antibiotic shortens its effective life. In commercial terms, antibiotics are “anti-capitalist commodities”: their value depletes with every dose. Unsurprisingly, major drug companies have abandoned the field.
The result is a tragic paradox. On the one hand, the world desperately needs new antibiotics to treat resistant infections. On the other, the market provides no incentive to discover them. The few that are developed are often priced cheaply, without accounting for the social cost of resistance. The externalities, like those of burning fossil fuels, are unpriced and therefore ignored.
Glimmers of hope: Science and innovation
There are signs of progress. Scientists are exploring alternative models, such as government-funded research institutes to produce publicly owned antibiotics, or “subscription models” where health systems pay companies a fixed amount regardless of usage, removing incentives for over-prescription. In the United Kingdom, the NHS is piloting such an approach.
New technologies are also opening doors. Researchers at MIT have used generative artificial intelligence to design two novel antibiotics—NG1 and DN1—capable of killing drug-resistant gonorrhea and MRSA in mice. These molecules are structurally distinct from any known antibiotic, targeting new bacterial proteins. If early promise translates into human trials, AI-guided discovery may become the most important tool in the fight against superbugs.
The way forward: A global compact
Antibiotic resistance mirrors climate change in its global inequality. High-income countries, after decades of abundant antibiotic use, are now urging restraint. Low- and middle-income nations, where infectious disease burdens are still high, demand access. The world cannot resolve this crisis without a global compact that balances equity with sustainability.
Three priorities stand out. First, surveillance and stewardship must improve. Antibiotics should not be available over the counter; prescriptions must be judicious, and usage in agriculture must be drastically curtailed.
Second, investments in public health infrastructure—sanitation, vaccination, and infection control—can reduce demand for antibiotics. The largest historical declines in infectious disease came from clean water and hygiene, not from new drugs.
Third, international financing mechanisms must support antibiotic research insulated from the failures of the market. Prizes, public-private partnerships, and nonprofit drug development consortia can play pivotal roles.
The antibiotic era is less than a century old, yet the reckless assumption of endless supply has brought it close to collapse. The comparison with fossil fuels is apt: both offered miraculous progress, both were squandered, and both now confront us with existential limits. But unlike fossil fuels, antibiotics cannot be phased out. They are the bedrock of modern medicine.
If nations fail to act, humanity risks a post-antibiotic world where childbirth, surgery, and routine infections carry deadly risks. The reckoning is already upon us. The task now is to slow the tide, invest in innovation, and build sustainable systems for the future. Antibiotic resistance is not a distant threat; it is the defining health crisis of this century.