


November 14, the birthday of Frederick Banting, who co-discovered insulin along with Charles Best in 1922, is observed as the UN-designated World Diabetes Day. The symbol for diabetes awareness is a blue circle. Access to Diabetes Care – If Not Now, When? is the theme for World Diabetes Day 2021-23.
When I teach public health, often I contrast health and medicine and say, health is outside the hospital.
“Do you want fries with that?” is a standard catchphrase asked by millions of fast-food restaurant workers every day to their customers. Similarly, a doctor treating diabetes may have to recommend social prescriptions with medical prescriptions. The magnitude of the disease burden and the pace with which diabetes is becoming more prevalent across the globe means that everyone must take note and act with greater urgency in all sectors of society.
READ I Fighting heavy odds: Corporate influence over policy weighs on India’s public health system
World Diabetes Day
A detailed analysis of the context and determinants of health and wellness are needed to develop a social prescription rather than simple advice of lifestyle modification, as diabetes is not an outcome of lifestyle choices alone. For instance, clinicians may wish to neglect the financial side of diabetes care and focus on less contentious and more familiar matters such as a call for lifestyle modifications.
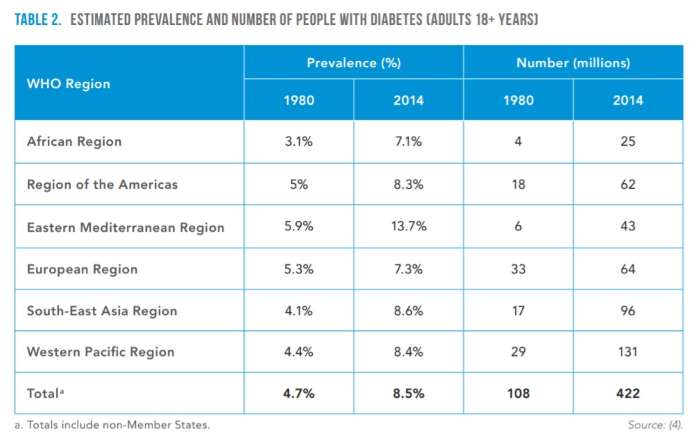
One in seven births — mostly young mothers- are affected by gestational diabetes. Moreover, diabetes prevalence is rapidly increasing in low- and middle-income countries than in high-income countries. In 2019, there were 1.5 million death was due to diabetes, according to WHO data. The number of people with diabetes rapidly rose from 108 million in 1980 to 422 million in 2014.
The International Diabetes Federation estimates that 72.9 million adults in India were living with diabetes in 2017. There are significant differences in diabetes prevalence between states in India. A 2017 study by Anjana RM et al. (2017) found that diabetes prevalence was higher in urban areas, and the overall prevalence of diabetes in 15 states of India was 7·3%. According to this study, the overall prevalence of pre-diabetes in these 15 states was 10·3%.
READ I Covid-19 lessons: Public health system must offer free drugs, diagnostics

The prevalence of diabetes varied from 4·3% in Bihar to 10·0% in Punjab and was higher in urban areas than in rural areas. Overall, 47·3% of individuals identified as having diabetes had not been diagnosed previously. An epidemiological transition is taking place with a higher prevalence of diabetes in low socio-economic status groups in the urban areas of the more economically developed states.
According to the US CDC, diabetes is now the seventh leading cause of death in the United States. More than 34 million people — including 13% of all adults — in the US have diabetes, with 90-95% of those cases being type 2. As per the US CDC (2020) data, the number of adults diagnosed with diabetes has more than doubled over the past 20 years, while 1 in 5 people with diabetes remain unaware that they have it. About a third of the entire US adult population (approximately 88 million people) have prediabetes, and 84% of them do not know about their own condition.
CDC data on youth with diabetes show that from 2001 to 2017, the number of people younger than 20 living with type 2 diabetes grew by 95%. The most significant increases in type 2 diabetes were in Black or Hispanic youth, and the highest number of youth per 1,000 living with type 2 diabetes was in Black or American Indian youth.

Diabetes is a significant cause of blindness, kidney failure, heart attacks, stroke and lower limb amputation. Between 2000 and 2016, there was a 5% increase in premature mortality from diabetes. In 2019, Diabetes was the ninth leading cause of death, with an estimated 1.5 million deaths directly caused by diabetes.
The health impact of uncontrolled diabetes is severe. Over time, diabetes can damage the heart, blood vessels, eyes, kidneys, and nerves. Adults with diabetes have a two- to three-fold increased risk of heart attacks and strokes.
Combined with reduced blood flow, neuropathy (nerve damage) in the feet increases the chance of foot ulcers, infection and the eventual need for limb amputation. Diabetic retinopathy is a significant cause of blindness and occurs due to long-term accumulated damage to the small blood vessels in the retina. Close to 1 million people are blind due to untreated diabetes. In addition, unmanaged diabetes is among the leading causes of kidney failure.
Healthy diet, physical activity key to prevention
According to WHO, a healthy diet, regular physical activity, maintaining an average body weight and avoiding tobacco use prevent or delay the onset of type 2 diabetes. In addition, diabetes can be treated and its consequences avoided or delayed with diet, physical activity, medication and regular screening and treatment for complications.
However, that is not the whole story. Healthy eating is imperative in preventing and treating diabetes. However, a healthy diet cannot readily be realised without access to affordable, nutritious foods. However, in a populous county like India, the number of poor people (with incomes of $2 or less a day) is estimated to have increased by 75 million because of the COVID-19 pandemic and associated recession. This accounts for nearly 60% of the global increase in poverty, an analysis by Pew Research Center revealed.

Likewise, an appropriate level of physical activity — a fundamental underpinning of health and wellbeing — becomes more difficult to achieve when limited by a lack of safe and accessible spaces for recreation or simply walking as part of daily life activities. Most public roads in developing countries do not have a footpath with roads and highways.
One limitation of public health data and analysis is that by only focusing on specific aspects of data, we miss the more significant impact disease can have on an individual and a society and how an individual’s life circumstances influence such chronic disease. We may make the mistake of reducing a disease to just an outcome of a few lifestyles.
The macro diabetes data may indicate the gravity of the situation. However, they do not fully explain the share of disease burden, enhanced morbidity and premature mortality associated with diabetes. Moreover, along with obesity, hypertension, and other common chronic conditions, diabetes dramatically increases the risk for adverse health outcomes when other comorbidities are present.
For these reasons, I would argue that diabetes is not just an outcome of certain lifestyle choices. Instead, it is a condition that also contributes to, and is impacted by, various other determinants of health such as structural, social, commercial, environmental, behavioural, and genetic determinants as well as access to affordable healthcare.
The Covid-19 pandemic illustrates the vulnerability of a person with diabetes to acquire infection and further complications. Those with pre-existing diabetes who are infected with the SARS-CoV-2 virus are more likely to experience worse complications and prolonged hospitalisation and are subject to higher mortality rates. Nearly 60% of all COVID-19 hospitalisations are attributable to a patient having diabetes, hypertension, and obesity combined.
Structural determinants of health are complex and multidimensional. Social structure is the patterned social arrangements in society that are both emergent from and determinant of the actions of individuals. Likewise, society is grouped into structurally-related groups or sets of roles with different functions, meanings, or purposes. Examples of social structure include family, religion, law, economy, and class.
Health is intricately woven into social structures and determined by the quality and density of structural relationships. For example, in many societies, pregnant women’s physical activities are restricted by religious belief, which has implications for gestational diabetes. Family and religion greatly influence the type and quality of food, which has a bearing on the advancement and control of diabetes. In addition, trade laws, economy, and class determine access to diabetes treatment and the quality of care and drive health inequities.
Similarly, social determinants of health — the conditions in which we are born, live, learn, work, play, and age — are significant drivers in the development and course of diabetes and other chronic illnesses. However, these factors are linked to a disproportionately increased risk for vulnerable people: older, cultural minorities, and socially marginalised populations.
Unlike many other health conditions, diabetes prevention, care and control has much to do with commercial determinants of health. According to WHO, commercial determinants of health are the conditions, actions and omissions by corporate and regulatory actors that affect health. Commercial determinants arise in providing goods or services for payment and include commercial activities and the environment in which commerce occurs. Consequently, they can have beneficial or detrimental impacts on health.
According to WHO, commercial determinants of health are the private sector activities that positively or negatively affect people’s health. In addition, the private sector influences the social, physical and cultural environments through business actions and societal engagements; for example, supply chains, labour conditions, product design and packaging, research funding, lobbying, preference shaping and others.
Commercial determinants of health impact a wide range of health outcomes, including diabetes, obesity, cardiovascular health, cancer, road traffic injuries, mental health and malaria. Commercial determinants of health affect everyone, but young people are especially at risk, and unhealthy commodities worsen pre-existing economic, social and racial inequities.
The development of therapeutic insulin in 1921 was a landmark breakthrough in the history of medicine. However, 100 years on, millions of lives have been saved and improved, but insulin and other diabetes medicines, diagnostics and care remain beyond the reach of many who need them.
For millions of people living with diabetes, access to insulin is a matter of life and death. Unfortunately, the average list price of insulin has skyrocketed in recent years. The reasons are partly due to the complexity of drug pricing in general and insulin pricing in particular, and many governments’ lack of political will to regulate the insulin price. In recent years, the widening gap between the net and list price of insulin is an example of political inaction to regulate insulin price, contributing to severe health inequity.
The social determinants of health are the circumstances in which people are born, grow up, live, work and age, and the systems to deal with illness. These circumstances are shaped by a broader set of forces: economics, social policies, politics, and the commercial determinants of health. Social determinants of health matter because addressing them helps prevent illness and promotes health, wellbeing and societal equity.
Diabetes prevention and treatment efforts, in primary care settings or at the territory care, fail to address inequities in social determinants of health — food insecurity, poor access to preventive health services, and lack of health-promoting school environments likely to be unsuccessful.
Any meaningful impact on the quality of life of people with diabetes hinges on improving the commercial and social determinants of health — which are often outside the realm of experience and training of clinical providers and the traditional healthcare system. In the simplest terms, determinants of health are outside the hospital, and a broader social, structural factory needs to be considered in developing public health response to a disease such as diabetes.
The process for establishing diabetes prevention and care depends on incorporating a comprehensive approach to understanding, charting, and acting on public health issues.
- Promote local community-based assessments to understand inequities across social, structural and economic determinants of health domains at the grassroots level,
- Improve health literacy and promote self-care in culturally sensitive ways,
- Support communities with programs relevant to their local needs that promote health and wellbeing.
To make significant, sustainable progress in preventing and treating diabetes as well as other chronic conditions, we cannot passively accept the health inequities that exist across this country and that have been contributing to the increase in the prevalence of chronic diseases
(Dr Joe Thomas is Professor of Public Health, Institute of Health and Management, Victoria, Australia. Opinions are personal.)
References:
CDC (2020) National Diabetes Statistics Report, 2020
Cefalu WT et al., (2018) Insulin Access and Affordability Working Group: Conclusions and Recommendations. Diabetes Care 2018 Jun; 41(6): 1299-1311.
Anjana RM, et al. (2017). Prevalence of Diabetes and prediabetes in 15 states of India: Results from the ICMR–INDIAB population-based cross-sectional study.
WHO (2021) Diabetes.
Pew Research Center analysis (2021) In the pandemic, India’s middle-class shrinks and poverty spreads while China sees smaller changes.